A prospective, randomized trial, STEMI Treated With Primary Angioplasty and Intravenous Lovenox or Unfractionated Heparin (ATOLL), presented at the European Society of Cardiology 2010 Congress strengthens the observational evidence that the low-molecular-weight heparin (LMWH), enoxaparin, is superior to unfractionated heparin (UFH) in primary percutaneous coronary intervention (PCI) for ST-elevation myocardial infarction (STEMI).
The trial randomized 910 patients undergoing PCI for acute STEMI (who did not receive any previous anticoagulation) at 43 centers in Austria, France, Germany and US to either of the following groups:
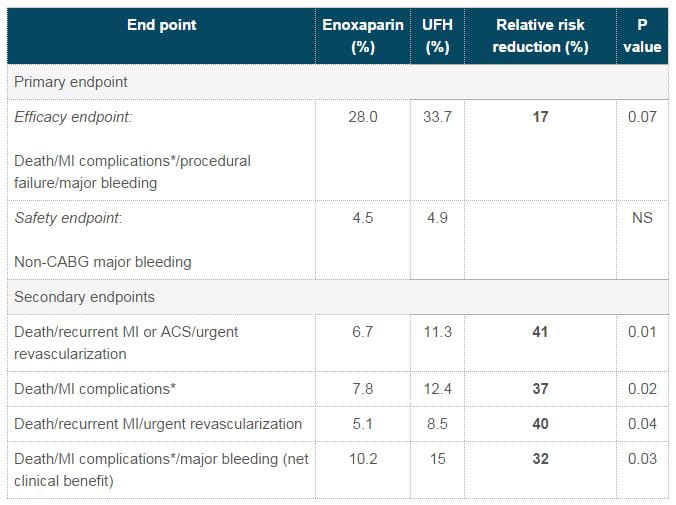
The primary endpoint (30-day composite outcome of death and major bleeding) was not significantly different between the two groups, although a favorable trend was observed in the enoxaparin group. On the other hand, enoxaparin was significantly superior to UFH in terms of the secondary end points (composites of serious clinical events) of the trial (Table 1).
The relative risk of death from any cause was 40% lower (p=0.08) and the composite rate of death or resuscitated cardiac arrest was significantly lowered by 42% (p<0.05) in the enoxaparin group vs UFH.
In spite of the fact that primary outcome was not significantly different with enoxaparin vs UFH, the trial investigators as well as discussants supported the superiority of IV enoxaparin over the traditional primary-PCI mainstay, UFH due to differences in the secondary endpoints. They further pointed that enoxaparin had inherent advantages over UFH which include bolus dosing and no need for measuring coagulation times.
ATOLL, according to Dr Gilles Montalescot, H-pital Piti-Salp-tri-re, France, the trial presenter; was a reliable test of enoxaparin as it included an especially high-risk primary PCI population (patients in shock, in cardiac arrest and with no age limit), one that closely reflected the kind of patients treated in the real world. Montalescot also mentioned that PCI was performed with radial-artery access in 2/3rd of study patients. He pointed that as radial access poses a much smaller risk of access-site bleeding compared with femoral-artery access; it probably might contribute to the non-significant difference for primary endpoint observed in the enoxaparin group.